If you spend any time inside looksmaxxing communities, you'll notice an odd pattern. The discourse is almost entirely face-coded — canthal tilt, midface ratio, gonial angle, buccal fat, maxillary projection. Frame gets mentioned, but it gets mentioned the way people mention the weather: something that exists, something that affects the experience, something you can't really do much about. That framing is wrong in a specific, testable way, and the reason it's wrong comes down to the clavicle.
The Visual Math Nobody Does
Here's an exercise. Take two men of identical facial harmony, identical height, identical body fat percentage, and identical muscle mass. Give one of them a biacromial width — the straight-line distance between the outer points of the shoulders — that sits at the 50th percentile for his height. Give the other a biacromial width at the 85th percentile. Now put them in the same t-shirt and photograph them from the front.
The second man looks better. Not marginally — categorically. His head looks smaller relative to his shoulders, his waist looks narrower by the same visual proportion, his posture reads as more dominant because the V-taper silhouette is itself a dominance signal across essentially every culture that has been studied. None of his facial features changed. None of his body fat or muscle mass changed. The only variable that moved was the width of a single bone.
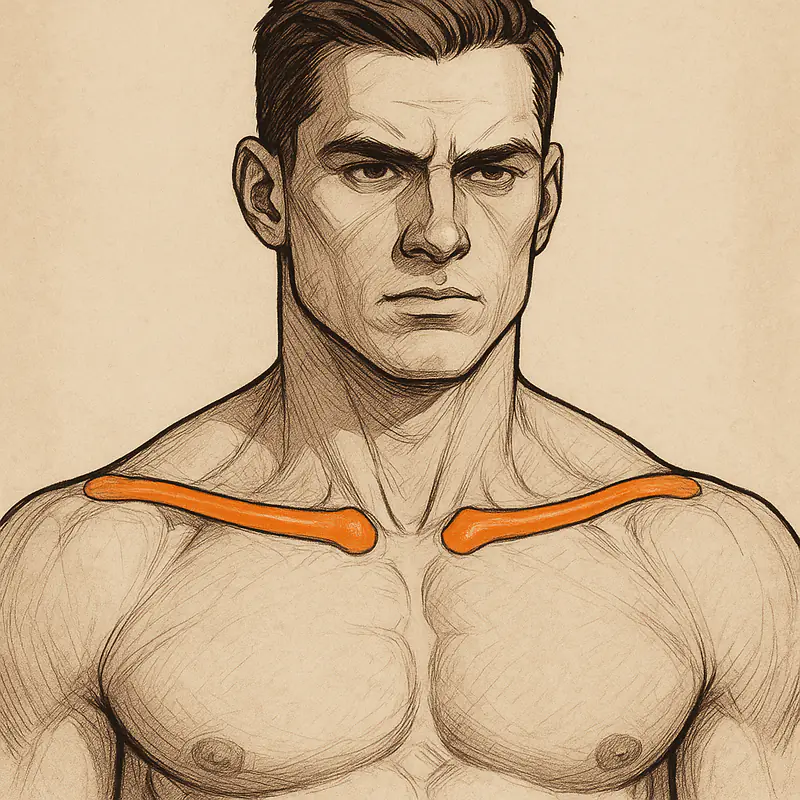
Biacromial width is substantially determined by clavicular length. The clavicle is the horizontal strut that sets how far the glenohumeral joint — the shoulder socket — sits from the midline. Two people with the same muscular development and the same deltoid size will look completely different if their clavicles differ by even a few centimeters. And because the visual effect compounds with muscularity — wider frame holds more mass better, and the mass it holds reads as more impressive — clavicular width is arguably the highest-leverage single variable in the entire male aesthetic package.
The reason looksmaxxing underweights it is simple: for most of the discourse's history, the assumption has been that clavicular width is fixed. It isn't, or at least it isn't as fixed as the assumption implies, and the published data on clavicular growth is clear enough that the fixed-frame assumption deserves to be retired.
The Growth Window Is Longer Than You Think
The medial clavicular epiphysis is the last growth plate in the human skeleton to fuse. Radiographic and CT studies put complete fusion somewhere between ages 23 and 27 in most individuals, with outliers extending toward 30. Longitudinal data on clavicular length shows meaningful elongation continuing well past the age at which general height has plateaued — in male subjects, on the order of 34 percent length gain between age 12 and age 25, a substantial portion of which occurs after age 18. Female fusion tends to run several years earlier.
What that means practically is that a 21-year-old man asking whether his frame is "done" is almost certainly asking a question with a biologically negative answer. His height is done. His facial bones are done. His clavicle very likely is not. The window during which a hormonal and mechanical loading protocol can plausibly influence clavicular elongation is open for years after most other structural variables have locked in.
The biological substrate is straightforward. Endochondral growth plates respond to the GH/IGF-1 axis. As long as the growth plate is open, chondrocyte proliferation at the physis is sensitive to growth factor signaling, and longitudinal bone elongation is the downstream outcome. After fusion, the mechanism shifts from elongation to periosteal apposition — the bone gets thicker in cross section rather than longer — and the leverage of hormonal intervention drops sharply.
The Peptide Categories With a Mechanistic Case
A looksmaxxing research protocol targeting clavicular development — meaning, for the individual, a protocol run during the individual's open-window years and designed to maximize the biological inputs to clavicular elongation — draws from three peptide categories, each addressing a different part of the biology.
Growth hormone secretagogues. The combination of CJC-1295, a growth hormone releasing hormone analog that extends the half-life of endogenous GHRH signaling, and ipamorelin, a selective ghrelin receptor agonist that produces clean GH pulses without elevating cortisol or prolactin, is the most discussed approach to amplifying the body's own GH output. The advantage over exogenous GH is that pulsatile release is preserved, negative feedback loops stay functional, and the risk profile is substantially lower. The disadvantage is that the effect is bounded by the individual's own pituitary capacity.
IGF-1 analogs. IGF-1 LR3 is a modified form of IGF-1 with an N-terminal extension that dramatically reduces its binding to the circulating IGF-binding proteins that normally sequester IGF-1 and limit its effective half-life. Native IGF-1 has an active window of roughly 10 to 12 minutes. IGF-1 LR3 extends that to 20 to 30 hours, producing sustained receptor activation across all IGF-1-sensitive tissues — including chondrocytes at an open growth plate. For individuals within the clavicular window, IGF-1 LR3 is the most direct available mechanism for stimulating endochondral growth at the target structure.
Connective tissue and recovery peptides. BPC-157 and TB-500 do not act directly on the physis, but they enable the training volumes that any mechanical loading protocol requires. BPC-157, a synthetic pentadecapeptide derived from gastric juice, has animal data supporting accelerated tendon, ligament, and soft tissue healing. TB-500, the synthetic fragment of thymosin beta-4, regulates actin polymerization and has a systemic recovery profile. Neither is a growth factor in the structural sense, but both extend the mechanical training ceiling that the growth factor environment is supposed to amplify.
Mechanical Loading Is the Signal
This is where a lot of protocols go wrong, and it's worth being explicit. Growth factor signaling does not produce localized skeletal adaptation on its own. Wolff's law is not optional. Bone responds to the mechanical loads imposed on it, and the GH/IGF-1 axis amplifies that response rather than substituting for it. A protocol that stacks the hormonal environment without loading the target structure is running only half of the intervention.
For the clavicle, the loading movements that transmit direct force through the structure are overhead pressing variations — barbell military press, seated dumbbell press, push press — which apply compressive and bending loads through the acromioclavicular joint and along the clavicular shaft. Heavy horizontal pulling, particularly rowing variations with controlled eccentrics, loads the sternoclavicular and AC joints through different vectors. Progressive overload across months is the substrate; weekly fluctuations are noise.
The muscular layer on top of the skeletal frame is the secondary variable. Lateral and rear deltoid development widens the visual silhouette beyond skeletal width alone, and trap development frames the clavicular region from above. None of these replace the underlying bone, but they compound the visual effect of whatever clavicular width the individual is working with.
Sourcing Is Not a Detail
For anyone running a serious peptide research protocol, sourcing is the variable that determines whether the protocol means anything at all. Research-grade peptide purity requires synthesis at 95 percent or above, verified by HPLC and mass spectrometry, with batch-specific certificates of analysis that tie a given vial back to the specific lot it came from. Below that standard, the research is not research — it is an experiment with unknown inputs.
Vendor selection is therefore a quality-control problem, not a price-comparison problem. Operations like Core Peptides, which maintain a published catalog of third-party-tested research compounds with lot-traceable documentation, represent the minimum baseline for serious work. Comparable batch-level testing and transparent documentation are also available from Verified Peptides, whose sourcing reputation in the research community has been built specifically around HPLC verification and active quality-control publication.
The reason this matters is not brand advocacy. It is that a protocol designed over weeks and executed over months is invalidated by a single vial of unverified material, and the cost of correcting for that invalidation is measured in months of lost time rather than dollars.
Window Assessment Comes First
The step that almost every looksmaxxing protocol conversation skips is the one that should come before any compound decision: imaging assessment of the individual's current clavicular ossification status. The Schmeling-Kellinghaus five-stage classification system maps the progression from unfused through active fusion to complete ossification, and an individual's current stage is the single best predictor of whether a protocol targeting endochondral growth has any biological substrate to act on.
An individual in stage 1 or stage 2 has an open physis and is working with the full biological opportunity. Stage 3 is a partially fused transitional state where some chondrocyte activity persists. Stages 4 and 5 represent effectively complete fusion, at which point the protocol should shift entirely from longitudinal growth strategies to periosteal thickening strategies — a different mechanism, a different set of expectations, and a different evaluation of what peptide categories are still relevant.
Chronological age is an unreliable proxy. Imaging is not optional for a serious protocol.
The Realistic Summary
Clavicular width is the highest-leverage single aesthetic variable in the male looksmaxxing conversation, and the assumption that it is fixed after puberty is wrong for a meaningful fraction of the young adult population. The medial clavicular growth plate remains open into the mid-twenties in most men, and both the hormonal biology and the mechanical loading response that govern growth at other physes remain operative at this site for that extended window. The peptide categories with a mechanistic case for influencing clavicular elongation — GH secretagogues, IGF-1 analogs, and connective tissue peptides that support training ceilings — are grounded in established bone biology, but the direct human evidence for the specific outcome remains thin, and should be treated as a research question rather than a guaranteed outcome.
None of this is magic. It is applied endocrinology, applied biomechanics, and applied sourcing quality, run across months rather than weeks, during a biological window that closes at a different age for every individual. The looksmaxxing community's underweighting of frame relative to face is a strategic error. The clavicle is the variable that makes everything else land.